Note: I’ll be traveling a lot the next three weeks, so posts will be sporadic. Thanks for your understanding!
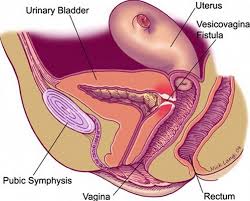
You’ve probably heard about the problem of obstetric fistula — the holes in between women’s pelvic organs that cause incontinence, pain, and social rejection. My own journey to becoming a doctor started when I first heard about this problem and the need for surgeons who could do procedures to cure fistula. (My skill set turned out to be more along the lines of preventing fistula, but that’s another story for another day!) Unfortunately, it turns out that they aren’t always as easy to fix as we thought, and sometimes the data are manipulated to bolster the reputations of organizations working to help these women:
How do these choices and calculations lead to notably distorted surgical “success” data? Let’s say one woman undergoes four surgeries in one year. The first three operations result in neither closure nor continence. In the fourth surgery, her fistula is successfully closed. Luckily, she is finally dry. Is this a case of one closure, one woman, and thus, 100 percent success? Or, is it one successful surgery in four with a 25 percent success rate? Maybe her fourth surgery closes her fistula but cannot restore her continence. In this scenario, is it 100 percent success, 25 percent, or 0? What if this woman, still incontinent, stays at the center for a second year and a fifth surgery? Since she didn’t leave the center in year one, perhaps she (and her four previous surgeries) do not even make it into the calculations for the year. These four surgeries, this woman, become statistically invisible. Given enough cases and enough data, it is easy to see how these different methods of calculating, manipulating, and reporting data could turn a 20–40 percent success rate into 80–90 percent.
So, why does this data manipulation matter? During my time in Niger, women underwent their first, second, fifth, and even eleventh surgeries only to be left with a persistent trickle of urine. Enveloped in a miasma of their own waste, and with their future fertility in question, it is easy to assume that women with fistula invariably become social pariahs within their home communities. And most media and humanitarian organizations do precisely this. Following an obstetric catastrophe, incontinent and with uncertain reproductive futures, these women are presented with a devastating set of eventualities by the standard media and humanitarian fistula narrative: divorced by their husbands and exiled from their communities. Yet, in contrast to the standard narrative of rejection and abandonment, for many of the women I came to know, it was not fistula itself that caused the greatest social harm. Too often, it was the prolonged search to cure it.
I don’t think we should necessarily stop providing free surgeries. But we do have to look at how prevention might be much more worthwhile, since the interventions needed to prevent fistula (like access to c-sections) are also the same sort of interventions that help prevent other perinatal morbidities and mortality.
Matthew Loftus
Matthew Loftus teaches and practices Family Medicine in Baltimore and East Africa. His work has been featured in Christianity Today, Comment, & First Things and he is a regular contributor for Christ and Pop Culture. You can learn more about his work and writing at www.MatthewAndMaggie.org
{kind=link}